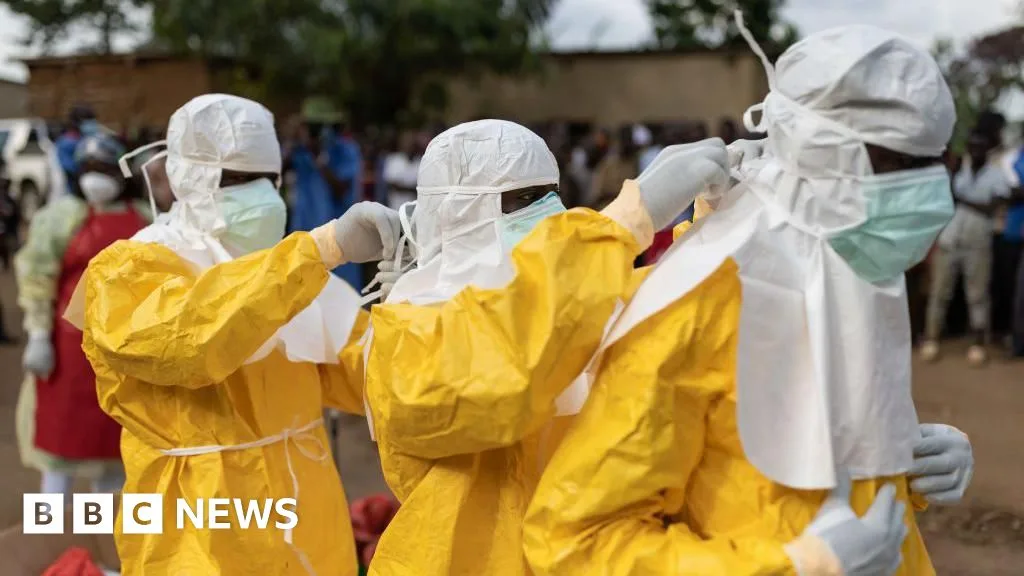
The World Health Organization declared the Ebola outbreak in eastern Democratic Republic of Congo's Ituri province and neighbouring Uganda a public health emergency of international concern on May 17, 2026 [1, 2, 3, 4]. The outbreak is caused by the Bundibugyo strain of Ebola virus, a rare species for which no approved vaccine or specific drug treatment currently exists [1, 5, 6, 7, 2, 3].
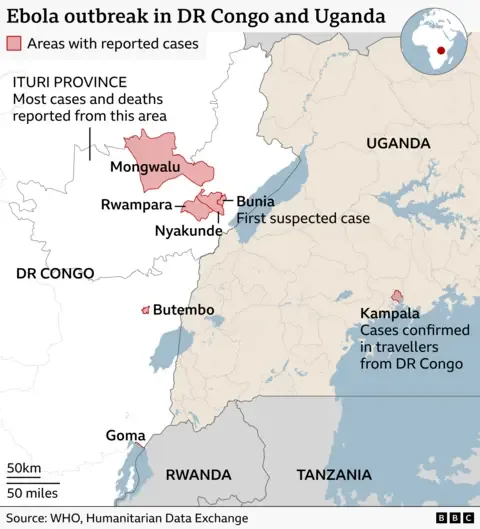
Since the presumed index case—a nurse—died on April 24 in Bunia, Ituri province, the virus has spread mainly in insecure, conflict-affected areas of eastern DR Congo including Ituri, North Kivu, South Kivu provinces, and the city of Goma [6, 8, 7, 2]. Around 513 suspected cases and between 131 and 139 deaths have been reported in DR Congo as of mid-May 2026 [8, 7, 9, 4]. Laboratory confirmation numbers remain limited, with eight confirmed cases as of early May [1, 2].
The virus has crossed borders, with confirmed cases and deaths now reported in Uganda [1, 8, 7, 2, 3]. Dr Anne Ancia, the WHO representative, said, "The more we are investigating this outbreak, the more we realise that it has already disseminated at least a little bit across border and also in other provinces" [8]. The infected virus spreads through direct contact with bodily fluids and contaminated surfaces, causing severe symptoms such as fever, vomiting, diarrhea, bleeding, and organ failure [1, 5, 6, 7, 3, 4].
The Democratic Republic of Congo's Health Minister Dr Samuel Roger Kamba acknowledged challenges at the community level, saying, "It means someone may have died before [the index case], or someone else may have been sick before him, but no one reported it" [7]. Dr Tedros Adhanom Ghebreyesus, WHO Director-General, warned there are "significant uncertainties to the true number of infected persons and geographic spread" [1].
Several countries have taken preventive steps. Rwanda closed its border with DR Congo, while Indonesia and Singapore have enhanced surveillance and public health measures at entry points to prevent imported cases [8, 3, 4]. The United States Centers for Disease Control and Prevention announced travel screening for passengers arriving from outbreak regions and restricted entry for non-US passport holders who recently traveled to Uganda, DR Congo, or South Sudan [10, 11, 12]. At least one American working in DR Congo has contracted Ebola and was evacuated to Germany, with at least six others being monitored or evacuated [8, 2, 10, 11, 12]. CDC Ebola response incident manager Satish Pillai said, "At this time, CDC assesses the immediate risk to the general US public as low" [10].
The outbreak’s occurrence in conflict zones complicates response efforts despite ongoing containment, and some international travel restrictions remain in place. The Democratic Republic of Congo canceled its pre-World Cup training camp in Kinshasa due to Ebola concerns, relocating preparations to Belgium [9].
Previous Bundibugyo Ebola outbreaks happened in 2007 and 2012, typically with a fatality rate of 30 to 33 percent, while overall Ebola fatality averages around 50 percent [1, 6, 7]. The WHO advises against closing borders or restricting trade with affected countries, stating such measures lack scientific basis and are often fear-driven [1].
The Ebola outbreak was first recognized after the nurse’s death on April 24 in Bunia. WHO’s emergency declaration followed on May 17, while the US CDC confirmed cases and implemented travel screenings by May 18 [6, 7, 2, 10, 11, 12]. Singapore announced stepped-up public health measures on May 19 in response to the emergency declaration [4].